The short answer:
Modern eyelid surgery is not simply about reducing tissue. The more important question is what should be preserved, released, repositioned, or supported so the eyelid looks brighter and more natural without becoming hollow.
Orbital Fat Is Part of the Eyelid Architecture
Orbital fat is the soft cushioning fat that sits around the eye within the bony socket. It helps protect the globe, but it also shapes what patients see in the mirror: upper eyelid fullness, the eyelid-brow junction, under-eye bags, tear trough hollows, and the transition from the lower eyelid into the cheek.
Older blepharoplasty thinking often treated orbital fat as a problem to remove. That can still be appropriate in selected cases, but it is not the whole story. Around the eye, volume is not automatically the enemy. Poorly positioned volume can create a bag; lost volume can create a hollow; and preserved or repositioned volume can create a smoother, more youthful contour.
This is why OFA-Bleph™ is planned around orbital fat as living structural tissue, not disposable filler. The aim is a rested eyelid that still has softness, projection, and natural movement. For a deeper look at how eyelid contour behaves in motion, read the EyeFACE Education™ guide to light, shadow, and movement in eyelid surgery.
If your main question is why the skin itself can look smoother after fat repositioning, the companion guide on fat support and under-eye skin quality explains how the layer beneath the skin can change the way the surface looks.
Orbital fat is structural
It supports the eyelid contour, cushions the eye, and helps create the soft transition between the eyelid, brow, orbital rim, and cheek.
Removal is permanent
Once orbital fat is aggressively removed, lost support can show up later as hollowing, sharper shadows, or a more operated appearance.
Repositioning can be powerful
In selected patients, orbital fat can be mobilized and transposed to soften hollows instead of discarding a useful autologous tissue.
Upper Blepharoplasty: The Eyelid-Brow Junction Matters
In the upper eyelid, patients often focus on hooding or excess skin. Dr. Gill also assesses brow position, crease height, levator function, ligament tethering, and the amount and position of orbital fat between the eye and the socket bone.
In selected patients, deep-plane ligament release and orbital fat transposition can support the upper eyelid-brow junction. This can act like an autologous natural filler effect: not a product placed under the skin, but the patient's own orbital fat used to restore soft volume, projection, and better light reflection.
Patients sometimes describe this as looking brighter, smoother, or more hydrated. The fat is not hydrating the skin like a cream; it is restoring the soft structural support that helps the upper eyelid reflect light in a healthier-looking way.
Lower Blepharoplasty: Bags and Hollows Are Usually Connected
Under-eye bags, tear trough hollows, and dark circles often come from the same three-dimensional problem. Orbital fat moves forward as a bag, while the tear trough below it catches shadow. If the fat is simply removed, the bulge may improve, but the hollow can become more obvious.
Lower OFA-Bleph™ commonly uses fat transposition: the patient's own lower eyelid fat is mobilized and repositioned over the orbital rim into the tear trough. The goal is to treat the bag and the hollow together, preserving useful volume while softening the lower lid-cheek transition.
This is especially important for patients searching for treatment of under-eye dark circles, hollows, or bags. If the darkness is structural shadowing, the solution may need to address contour, not only skin colour.
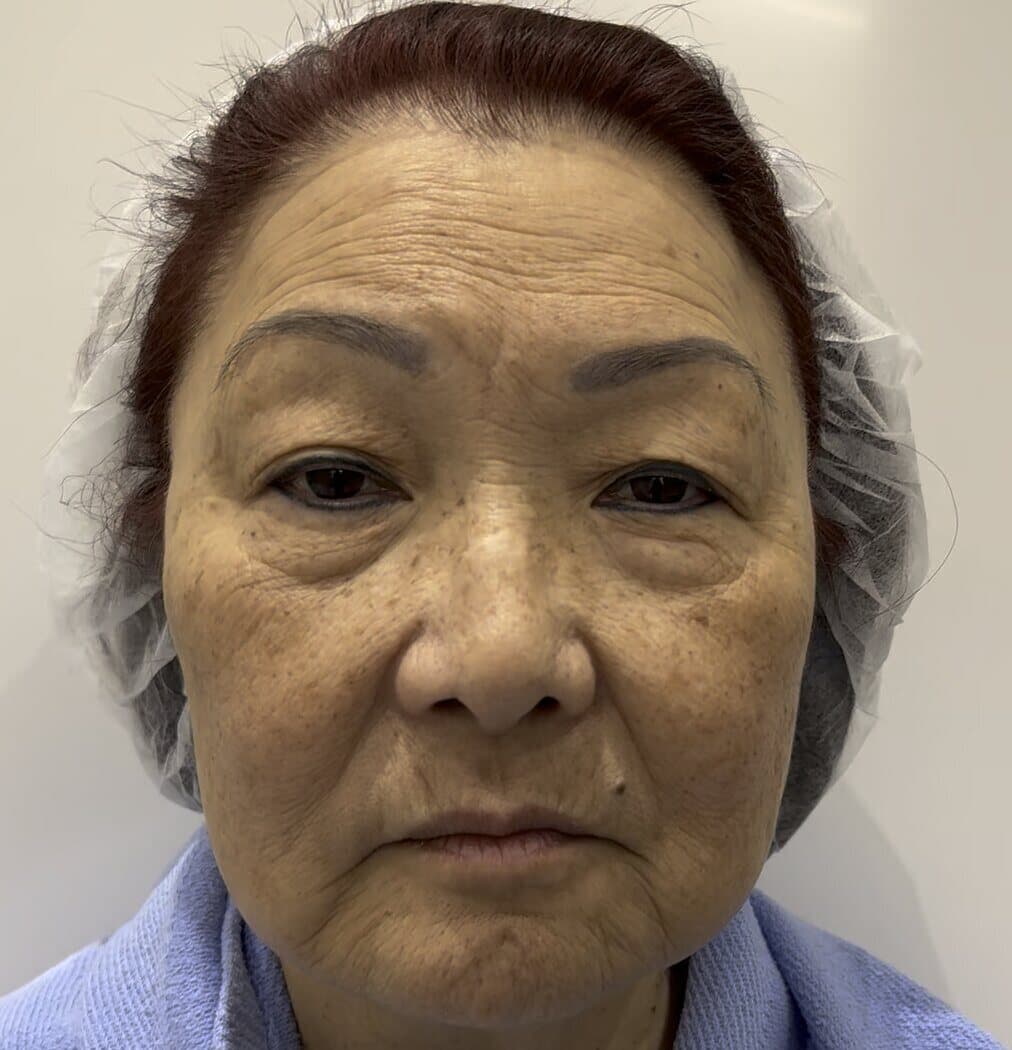
 pre-treatment
pre-treatment 8.5 months post-treatment
8.5 months post-treatmentLower OFA-Bleph™ Case Example
Using orbital fat to soften the bag-hollow pattern
This case shows why orbital fat can be useful tissue. The lower eyelid bag and the hollow below it create a shadowed transition. Repositioning the patient's own orbital fat can soften that transition while preserving a natural eye shape.
- The goal is contour correction, not simply reducing volume.
- The lid-cheek transition becomes softer.
- The goal is a result that remains recognizable and natural to the patient.
Educational example only. Individual anatomy, healing, and results vary.
How OFA-Bleph™ Uses Orbital Fat Differently
Upper OFA-Bleph™
Heavy upper lids, hooding, eyelid fold shape, upper-lid hollowing, and the eyelid-brow junction.
Deep-plane release, conservative reduction, and selective orbital fat transposition may be used to support the upper eyelid-brow complex when anatomy supports it.
Lower OFA-Bleph™
Under-eye bags, tear trough hollows, dark-circle shadowing, and the lower lid-cheek transition.
Vascularized orbital fat is often repositioned over the orbital rim to treat the bag and the hollow together, usually through a transconjunctival approach when appropriate.
Four-Lid OFA-Bleph™
The full eyelid frame: upper-lid platform, eye shape, lower-lid contour, brow support, and cheek transition.
Upper and lower planning are coordinated so the eyelids look refreshed together rather than reduced in separate isolated zones.
 pre-treatment
pre-treatment 5 months post-treatment
5 months post-treatmentRERF-M Case Example
When eyelid contour depends on midface support
Some lower eyelid concerns are not isolated eyelid problems. This four-lid OFA-Bleph™ and RERF-M example is included because the midface, lower eyelid, and lid-cheek transition move together.
- Midface support changes the lower eyelid-cheek transition.
- Hidden endoscopic access avoids visible facial scars.
- The result should work in motion, not only in still photographs.
Educational example only. Individual anatomy, healing, and results vary.
Why Not Just Use Filler?
Filler can be useful in carefully selected patients, but it is not the same as repositioning orbital fat. Filler adds synthetic volume. Fat transposition reuses a tissue already present in the eyelid and moves it into a more useful position.
The right choice depends on anatomy. Some patients need skin quality work, some need filler dissolved, some need lower eyelid fat transposition, and some need a broader plan involving brow or midface support. The consultation is where those categories are separated.
Questions to Ask Before Eyelid Surgery
- Am I a preservation, repositioning, or reduction case?
- Is my concern mainly skin, fat, brow position, ptosis, tear trough hollowing, or cheek support?
- If fat is removed, what prevents a hollow upper lid or sharper lower-lid shadow later?
- Can my own orbital fat be used as part of the contour plan?
- Will surgery improve the structural shadow, or is pigmentation/skin quality the bigger issue?
The EyeFACE Point of View
Dr. Gill is an ASOPRS fellowship-trained oculofacial plastic surgeon. His blepharoplasty planning starts with eye-surgery anatomy: eyelid position, blink, tear film, orbital support, brow position, lower lid tone, and facial balance.
OFA-Bleph™ is the expression of that philosophy. It is not reduction-only eyelid surgery. It is eyelid surgery planned around preservation, release, repositioning, support, and long-term naturalness.